Research Inequality in Nanomedicine
Abstract
The 10-90 gap is an idea in the healthcare literature that less than 10%of all research funding goes to solving health problems that are 90%of the global disease burden. This paper examines whether there is inequality in nanotechnology healthcare research(nanomedicine). To understand the inequality in nanomedicine, I conducted a bibliometric review of Web of Science and PubMed databases. Overall there is not large inequality in nanomedicine research. The bibliometric analysis shows that most nanomedicine research is done in high-income countries, but their research portfolios extend beyond rich world diseases like Alzheimer’s disease and diabetes to include research on malaria, tuberculosis, and HIV/AIDS. Of the nanomedicine articles that are directed towards specific diseases (about 20% in Web of Science and PubMed), the majority of the research (86%) will help both the rich and the poor, while only 7%of the research focuses solely on rich world diseases and 7% focus solely on diseases of poverty. The most researched nanomedicine topic is cancer. It accounts for 16% of nanomedicine literature. Overall less than 20% of nanomedicine research goes to solving health problems that are 50% of the global disease burden. Given nanotechnology is so linked to chemistry and the chemicals industry, the inequality within nanomedicine will impact how those industries supply materials, supplies, and information to the various stakeholders involved in nanotechnology and healthcare.
1 Background/Literature Review
Access to health care is a basic human right and over the past twenty years, healthcare has become a focus of development and aid organizations. One major initiative to improve global health is the United Nations’ (UN) Millennium Development Goals (MDGs) that were adopted in 2000. The MDG’s outline eight different poverty arenas that the world community wants to alleviate by 2015 (United Nations, 2010a). Three of the goals, child health, maternal health, and HIV/AID, deal directly with healthcare. With regards to child health, the UN wants to reduce under five-child mortality rate by two-thirds by focusing on decreasing pneumonia, diarrhea, and measles. For maternal health, the MDG is to reduce the maternal mortality ratio by three-quarters and ensure that every woman has access to pre-and postnatal care. Finally, the world community has committed to halting and reversing the spread of HIV/AIDS. It’s estimated that HIV/AIDS is the 6th most deadly disease and that the disease kills 2 million people each year (World Health Organization, 2008).
Despite efforts to improve the health of the indigent, the poor live a greater proportion of their lives sick compared to the rich and they have significantly lower life expectancy than the rich (World Health Organization, 2008). A potential cause of the health disparity is that there is not much research on diseases that affect the poor. The Global Forum for Health Research came up with the term the 10/90 gap to describe the inequalities in health research funding (Global Forum for Health Research, 2004). The 10/90 gap refers to the phenomenon that less than 10% of research funding goes to studying diseases that are 90% of the disease burden. Since 1990, the Global Forum for Health Research has brought awareness to the 10/90 gap by producing reports that track research disparity and engaging with the public and media about the problem. A report by the Médecins Sans Frontières found that health research expenditures are still heavily imbalanced. Four major diseases in developing countries tuberculosis, leishmaniasis, malaria, and trypanosomiasis are 5% of the global disease burden, but research expenditures for this disease are 0.1% of global health R&D (Global Forum for Health Research, 2004; Médecins Sans Frontières, 2001). Other studies have discussed the 10/90 gap in other healthcare arenas like medicines(Reich, 2000), female healthcare research (Doyal, 2004), cardiovascular diseases research (Martini et al., 2003), and healthcare publications (Mari et al., 2010; Pastrana et al., 2010). In general, these studies reach similar conclusions as to the Global Health Forum and Médecins Sans Frontières; medicine and health R&D are unequal and that society needs major reforms to fix the problem.
Compared to income and education inequality, health inequality is particularly dangerous because unlike other problems facing society, diseases can easily jump borders and spread around the world. Bacteria and infections are not biased; they can infect the rich and poor, global north and global south. In the past century rich countries undertook vast campaigns to eradicate several diseases like malaria and mumps. However, if the diseases are not treated in other parts of the world, they could reemerge in healthier nations. Recently The National Institute of Allergy and Infectious Disease in the USA identified five reemerging diseases including the mumps virus, streptococcus (strep throat), staphylococcus aureus (staph infection) (NIH, 2010).
However the legitimacy of the 10/90 gap has been challenged (Stevens, 2007). The opponents of the 10/90 gap argue that the poor’s higher mortality rates have little to do with research portfolios, but rather other social conditions that prevent the poor from getting the necessary treatment. The opponents cite that most individuals in developing countries do not die from obscure diseases, but rather from more common illnesses like lower respiratory infections and heart disease. These diseases afflict both the rich and the poor (World Health Organization, 2008) and hence it is an exaggeration to say that 90% of all research funding goes to solving the problems of the rich. Moreover, critics note that other major killers of the poor, like malaria and diarrheal diseases, have been thoroughly studied and many medicines exist to treat these ailments. Individuals die from these diseases because of other societal factors that prevent treatment, not from a lack of research. Finally the opponents of the 10/90 problem state that many organizations, like the Infectious Disease Research Institute, study diseases of poverty and hence there is not a dearth of research on neglected diseases (Stevens, 2007).
This paper investigates the 10/90 gap in relation to nanotechnology. Many believe that nanotechnology is the next big research trend. One scholar, Mohamed Hassan (2005), says that “nanotechnology could prove to be a ‘transformative technology comparable in its impact to the steam engine in the 18th century, electricity in the 20th century, and the Internet in contemporary society” (Hassan, 2005). As a result many countries, especially poorer countries, are heavily investing in the technology. A study conducted by Salamanca-Buentello et al. (2005) outlines ten different nanotechnologies that will help the world’s poor. Three of the ten technologies, disease diagnosis, drug delivery, and health monitoring, deal with healthcare issues (Salamanca-Buentello, 2005).
There is often confusion in defining nanotechnology (Balogh, 2010). This paper uses the National Nanotechnology Initiative definition of nanotechnology which “is the understanding and control of matter at dimensions between approximately 1 and 100 nanometers, where unique phenomena enable novel applications. Encompassing nanoscale science, engineering, and technology, nanotechnology involves imaging, measuring, modeling, and manipulating matter at this length scale” (PCAST, 2010). At the nanoscale, the matter has different properties, like conductivity and reactivity, which make it possible to do novel research and create new products. Central to nanotechnology is chemistry. Chemistry specializes in manipulating atoms andmolecules to create new substances (Whitesides, 2005). Without chemistry, nanotechnology and hence nanomedicine, could not exist as an emerging technology.
It is estimated that in 2005 there were 38 nano-enabled medical products with sales of about $6.8 billion, over 150 companies working in nanomedicine. This market was expected to double by 2012 (Wagner, Dullaart, Bock,& Zweck, 2006). In addition to these products, the field of nanotechnology will have a variety of economic impacts like increasing the productivity of manufacturing, creating a bigger market for scientists familiar with nanotechnology, and increasing competition between sectors (Zawislak, Marques, Esteves,& Rublescki, 2010). Chemistry and chemical companies are also expected to benefit from the increased emphasis on nanomedicine. Chemical companies supply many of the materials and equipment to conduct nanomedicine research. Moreover chemists are often used in nanotechnology labs to do research. (Zawislak et al., 2010). Hence it is important for chemists and chemical businesses to understand nanomedicine in order to participate in this new emerging field and market.
2 Research Problem
Though there is some agreement that nanotechnology can help the world’s poor, is there poverty-related nanotechnology research being conducted or is all the research geared to the problems of the rich and luxury goods? Is the 10/90 gap strong in nanomedicine or is the gap a different ratio? This study is a descriptive investigation of research intensity in nanomedicine and inequality in nanomedicine research.
There are three factors of nanomedicine inequality. First inequality in nanomedicine occurs between the different income levels of countries. Do very high-income countries dominate the research or is the research occurring equally across the world? The global distribution of nanomedicine is affected by two competing trends. Scholars have observed that nanotechnology research is taking place in both rich and poor countries. Many poor countries view nanotechnology as the next technology revolution so they are investing in the field early so they will not be left behind (Hassan, 2005). As a result, it is expected that nanomedicine research will be done in low-income countries. However medical research is still dominated by rich countries (Médecins Sans Frontières, 2001) and therefore it is also likely that nanomedicine will follow the same trend as general medical research.
Hypothesis 1: Nanomedicine research is predominantly conducted in very high-income countries
The second factor of inequality in nanomedicine is whether it focuses on diseases of very high income or low-income countries. The current literature on the 10/90 gap supports the idea that medical research will focus on diseases of the rich. Moreover, much of the medical research is funded by governments. Since the very high-income countries invest more in R&D than mediumand low-income countries, it is expected that most of the money will focus on problems that affect those countries.
Hypothesis 2: There is a disproportionate amount of nanotechnology research conducted on diseases of very high-income countries as opposed to the diseases of other countries
The third factor of inequality is whether researchers are focusing on the most dangerous diseases or are their attentions drawn to diseases that cause relatively few deaths. The literature suggests that research is focused on diseases that cause relatively few deaths while neglecting diseases that cause a lot of deaths (Global Forum for Health Research, 2004).
H1.3 The majority of nanomedicine research will only address diseases that kill relatively few people.
This study fills a gap in the literature. Most other studies discuss the societal and ethical implications (SEI) of nanotechnology and describe potential problems that may arise because of it (ETC Group 2006; Meridian Institute, 2006; Roco & Bainbridge, 2005). But there are few articles that quantitatively analyze inequality in nanotechnology research. This paper, on the other hand, examines the actually trends in nanomedicine research to determine if scientists are studying nanotechnology for the poor. In addition, this study not only explores where the research is being conducted, but it analyzes the content of the publications to determine which diseases are receiving themost attention.
3 Methods
To analyze inequality in nanomedicine research, I conducted a bibliometric examination of Web of Science (WoS) and PubMed databases. Web of Science is one of the largest publication databases. It contains over 13,000 journals in 200 disciplines ranging from 1900 until today (Thomson Reuters, 2012). WoS is a prominent database used by bibliometricians (Leydesdorff, 2008) to study publication and collaboration patterns in diverse topics like including tropical medicine (Falagas, Karavasiou,& Bliziotis, 2006), nano/biosensors (Huang, Peng, Guo, & Porter, 2010) and emerging technologies (S. Cozzens et al., 2010). My analysis is based on a nanotechnology database created by a group of researchers at the Georgia Institute of Technology (Porter, Youtie, Shapira,& Schoeneck, 2007). The database contains a list of all the nanotechnology articles in WoS. The team created the database by using eight Boolean logical search phrases to find the nanotechnology articles and then they used a second list of keywords to remove extraneous articles from their search. The database contains articles ranging from 1990-2012, but this study limits its scope to nanotechnology publications from 2000-2010. From 2000-2010, there are about 617,000 nanotechnology articles.
The second database used in this study is PubMed, a free online digital database of biomedical journal articles developed by the National Center for Biotechnology Information in the U.S. PubMed is a smaller database than WoS, but it is geared towards biomedical and health care related articles. The major component of PubMed is a database called Medline which has about 5,400 journals dating back to 1948 (National Center for Biotechnology Information, 2012). After accessing PubMed, I searched for nanotechnology articles in the database using a similar version of the Porter et al (2007) strategy. The PubMed search yielded 56,000 nanotechnology articles.
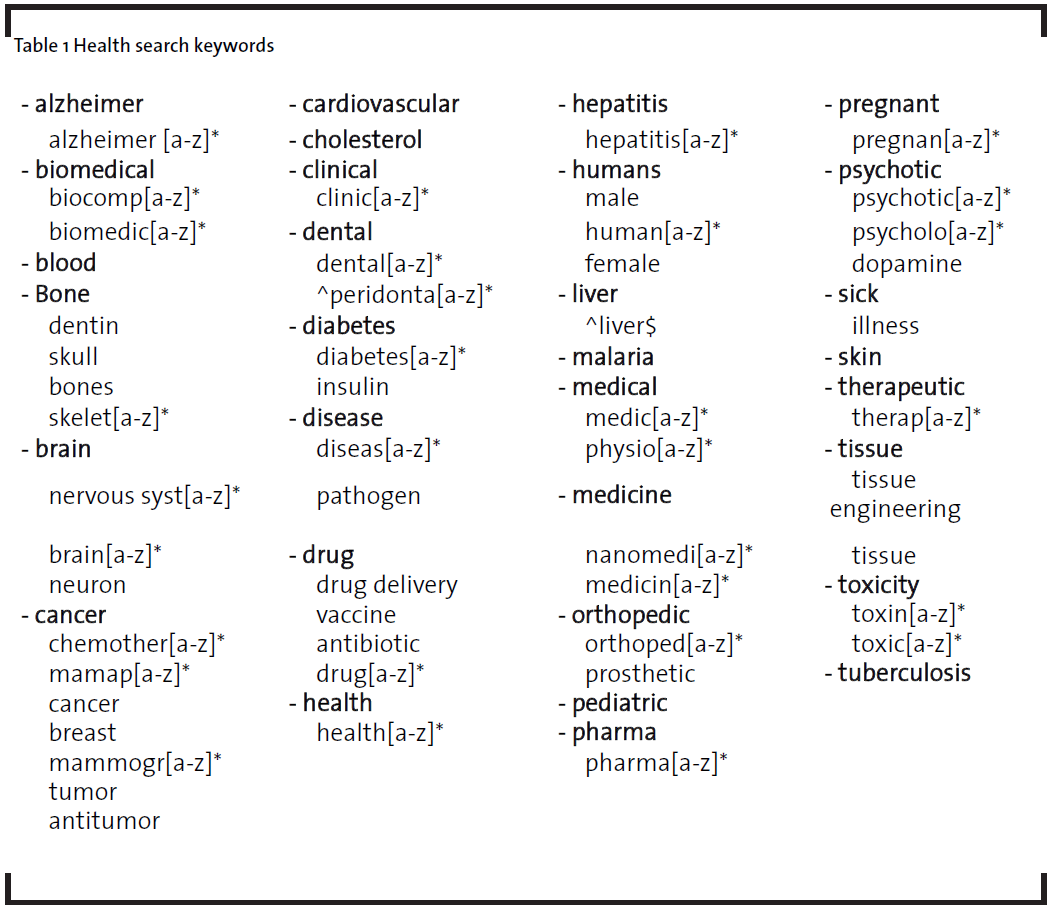
After the two nanotechnology databases were created, I developed a search strategy to find the health related articles by reading several nanomedicine review articles (ETC Group, 2006; OECD, 2005; Sahoo, Parveen,& Panda, 2007; Silva, 2004). These articles gave the keywords to formulate the health filter. See Table 1 for the list of keywords. Out of the 617,000 nanotechnology articles in WoS, 12% relate to nanomedicine; in PubMed, 48% of the 118,000 nanotechnology article relate to medicine.
Like all databases, WoS and PubMed have their limitations. These databases have a greater representation of journals from rich, western countries compared to developing countries, and these databases bias towards journals that are in English (UNESCO, 2005). Moreover the databases do not have 100% coverage of all the journals and so some publications that are not indexed in Web of Science or PubMed will be absent from the study.
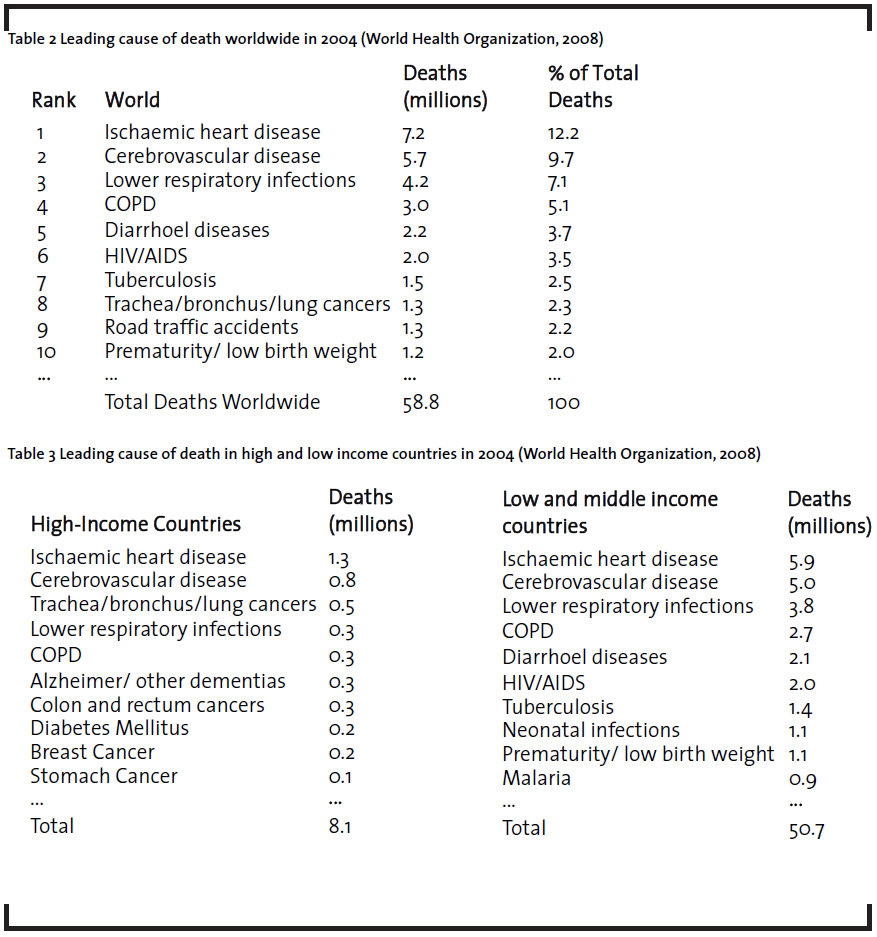
The 10/90 gap refers to the observation in the 1990’s that less than 10% of research funding went towards researching health problems that account for 90% of the global disease burden (Global Forum for Health Research, 2004). For this study, the global disease burden was based the mortality rates of the top diseases around the world. In 2008 the World Health Organization (WHO) updated a 2004 study that measured the top diseases based on their mortality rates. The WHO also classified the diseases based on a variety of factors including the mortality rates of the diseases in high, middle, and low-income countries (World Health Organization, 2008). Table 2 shows that top ten causes of death worldwide and Table 3 shows the top diseases in high and low-income countries income countries. The leading causes of death in the rich world come from illnesses like Alzheimer’s disease, lung, colon, breast, and stomach cancers, and diabetes. In poor countries, a large percent of the population die from diarrheal diseases, HIV/AIDS, tuberculosis, and malaria. There are four diseases, ischaemic heart diseases, cerebrovascular disease, lower respiratory infection, and COPD, that are common in both high-income and low-income countries. The list of diseases from the World Health Organization’s Burden of Disease report was used to develop a search filter to find diseases in the nanomedicine database and to classify the diseases as high-income or low income country diseases (World Health Organization, 2008).
Finally this study classifies countries using the 2011 United Nations Human Development Index (UN-HDI). The UN-HDI groups countries into four categories, very high development, high development, medium development, and low development, by using three dimensions, health, education levels, and living standards to develop a composite measure of the countries and then ranks them (United Nations, 2010b).
4 Results
4.1 Data Description
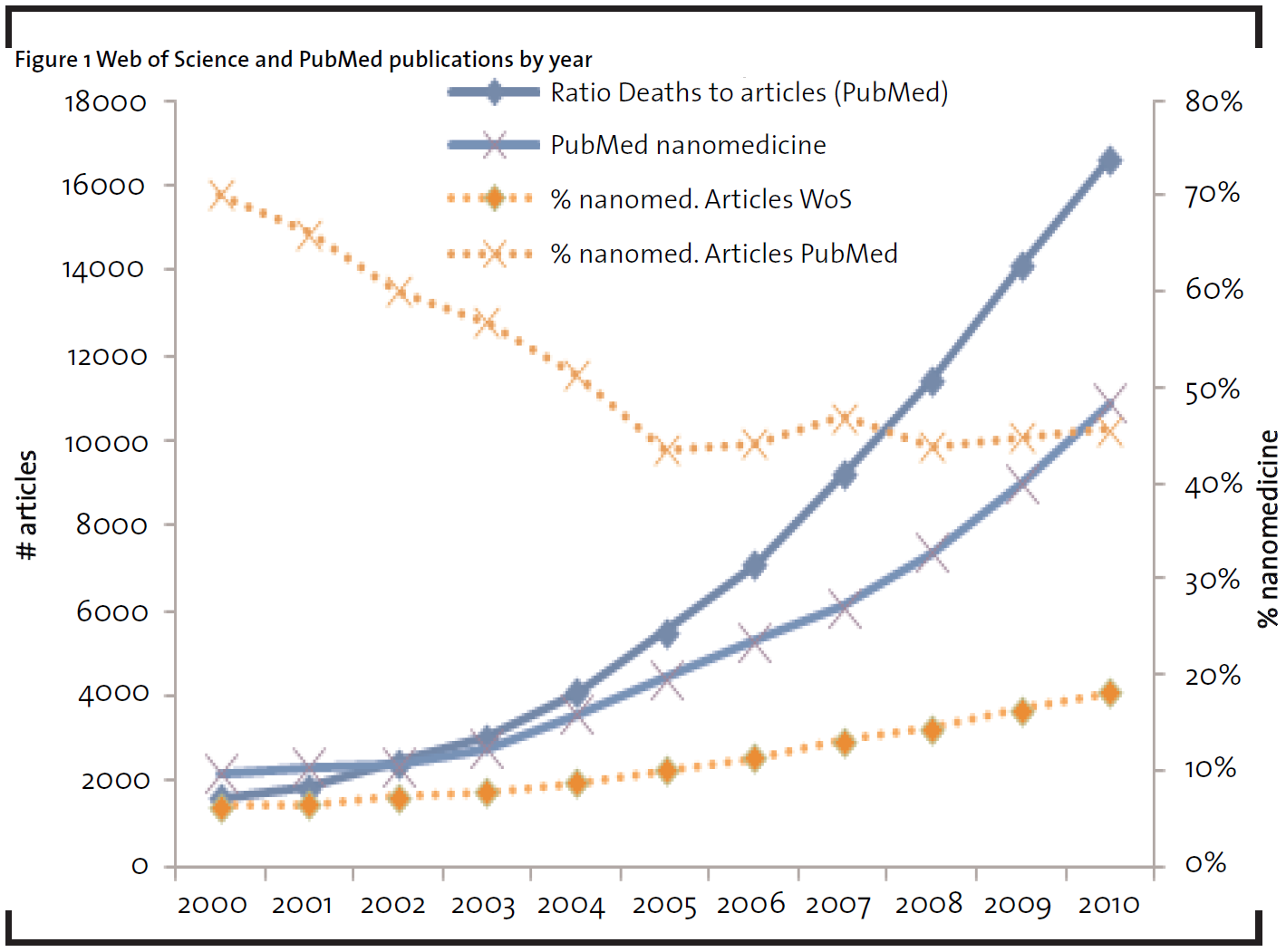
Below is the summary data from the nanomedicine database. WoS contains 77,078 nanomedicine articles and PubMed contains 63,653 nanomedicine articles from 2000-2010. In those 11 years, both PubMed and WoS had a steady increase in the number of nanomedicine articles. However, the databases contain different relative amounts of nanomedicine publications (see right axis of Figure 1). In PubMed more than 50% of the nanotechnology articles relate to nanomedicine while in WoS between 10% and 20% of nanotechnology articles relate to nanomedicine. It’s not surprising that PubMed has relatively more nanomedicine article compared to WoS because the database focuses on biomedical journals. The percent of nanomedicine articles in WoS increase from 10% to 20% from 2000 to 2010. In 2000, 70% of nanotechnology articles in PubMed related to nanomedicine. However, by 2005 the percent of nanomedicine articles in PubMed fell to 50%.
4.2 Country level inequality
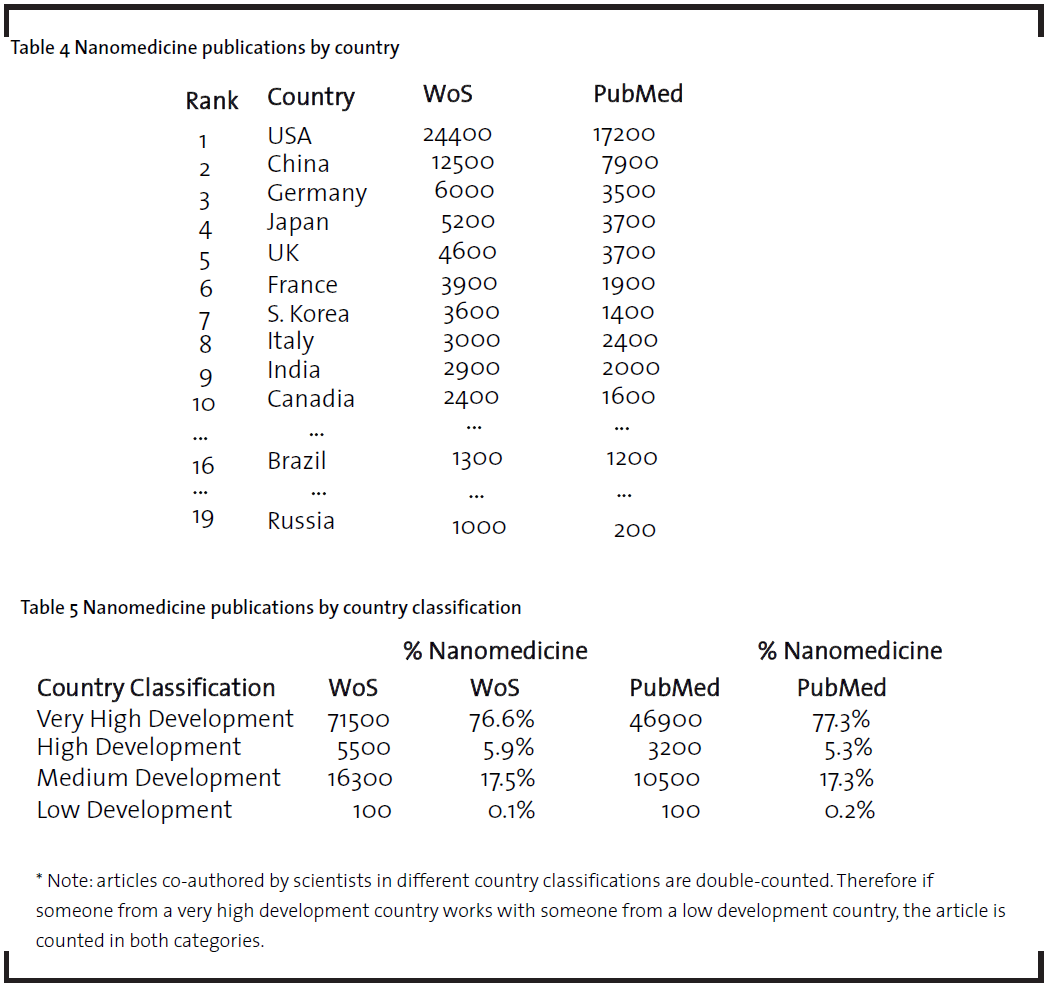
Table 4 is a list of the top countries publishing nanomedicine articles. In general, very high income countries like the USA, Germany, UK, and Japan published the most nanomedicine articles. However there are several emerging economies that also publish a lot of nanomedicine research. Most notably, China and India rank within the top ten countries for nanomedicine publications. In both the PubMed and Web of Science, China has the second most nanomedicine publications. China’s prominence in nanomedicine research is not unexpected. It is estimated that China spent over $250 million on nanotechnology in 2008 (Liu et al., 2009) and that it has over 30 institutions conducting nanotechnology research (Niosi & Reid, 2007). Moreover, other studies have also confirmed that China is a world leader in nanotechnology (Guan & Ma, 2007; Liu et al., 2009). India ranks tenth in nanomedicine publications in WoS and seventh in PubMed. Since 2001, India has formally invested in nanotechnology. In 2007 India started the NanoMission and they committed US $230 million to nanotechnology (Ramani, Chowdhury, Roger, & Reid, 2010). Other emerging economies like Brazil, Russia, Turkey and Iran rank within the top 25 nanomedicine publications in WoS or PubMed.
Table 5 classifies the countries based on the 2011 United Nations Human Development Index. There is a clear research gap between the different country classifications. The majority of nanomedicine research is conducted in very high income countries (about 77%) while the high, medium and low income countries lag behind. Medium development countries have the second highest nanomedicine publication count followed by high and low development countries. The productivity of medium countries is led by China and India which are classified as medium developed countries.
4.3 Disease research inequality
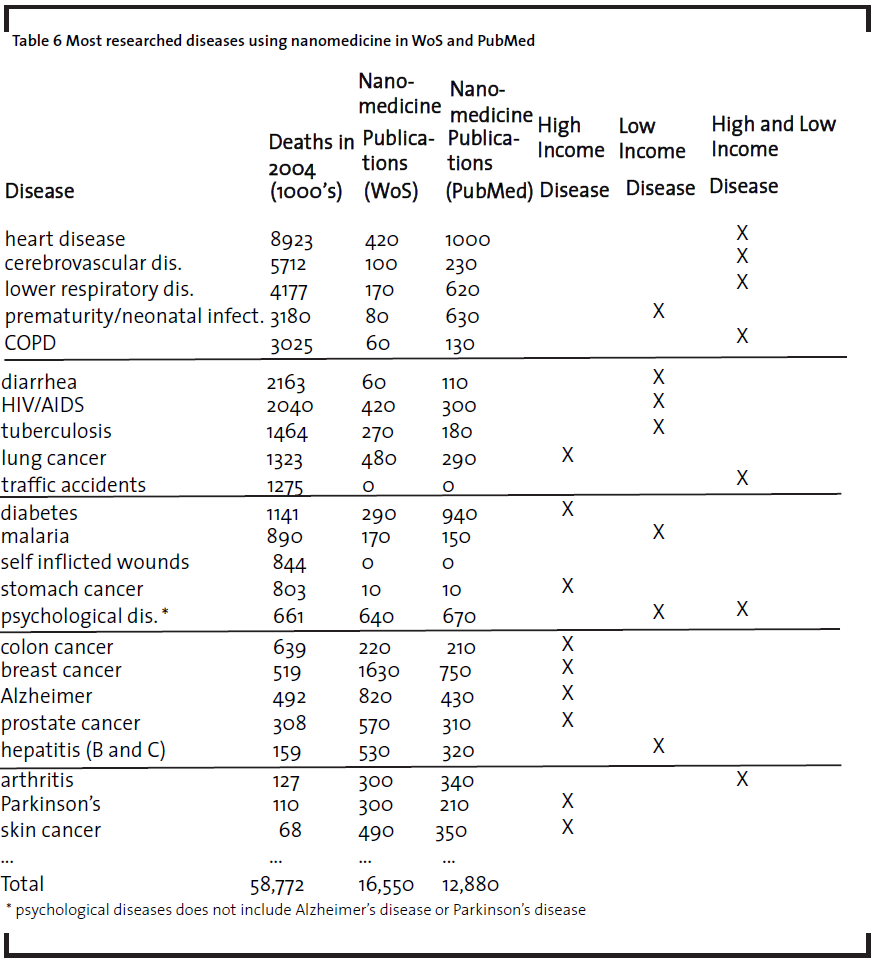
Nanomedicine, like other scientific fields, contains both basic and applied research. Much of the current literature in nanomedicine is basic research and does not apply to a specific disease. Using the top diseases found in the World Health Organizations Burden of Disease report as a guide for prominent world diseases, this study finds that about 20% of nanomedicine publications were directed towards a particular illness. The rest of the nanomedicine research was not directed towards fixing a specific disease. Table 6 lists the top researched diseases in nanomedicine. High-income country diseases are illnesses like Alzheimer’s and diabetes while low income country diseases are diarrheal diseases, HIV/AIDS, tuberculosis, malaria, and neonatal infections/deaths from prematurity. Common to both groups are cancer, heart disease, cerebrovascular disease, respiratory infection, and chronic obstructive pulmonary disease (COPD).
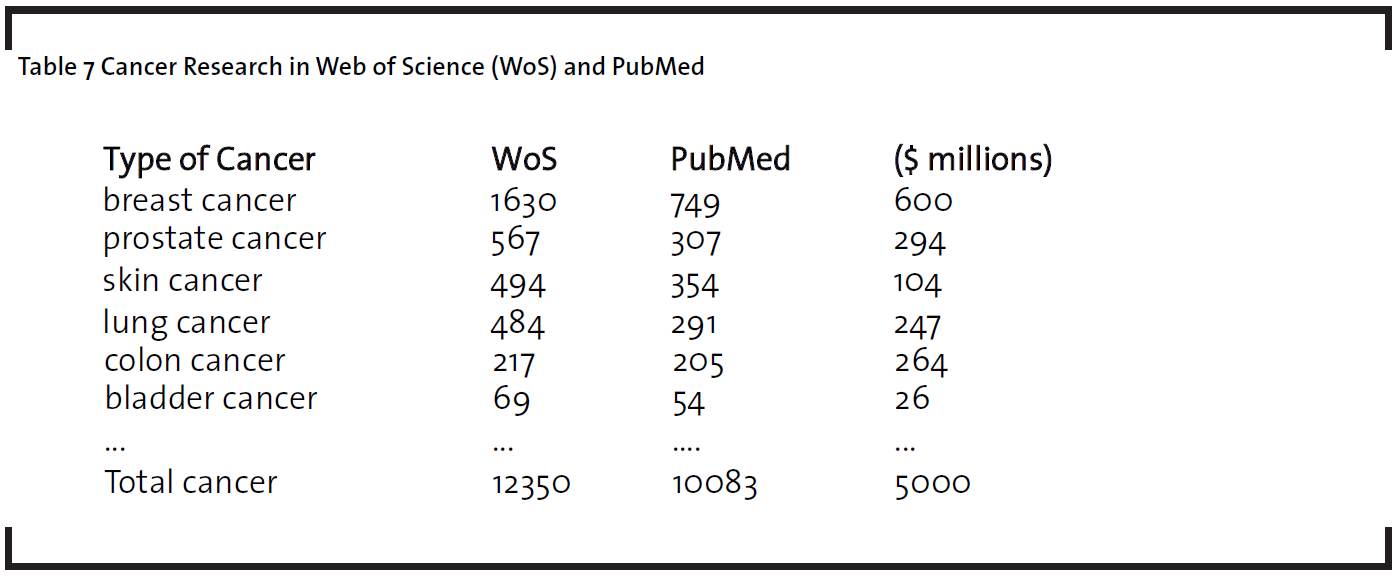
The disease with the most research publications in both WoS and PubMed is cancer. In both databases, cancer accounts for 16% of all nanomedicine publications and about 75% of the directed nanomedicine research. Cancer is a major cause of death, but the strong emphasis on cancer over exaggerates its burden of disease. It is estimated that cancer causes 12% of deaths worldwide (World Health Organization, 2008). For men, the most deadly type of cancer is lung and trachea cancer while breast cancer is the deadliest type of cancer for women. Over the past decade, governments and foundations invested a lot of money in cancer research. For example, in 2009, the National Cancer Institute (NCI) disbursed $5 billion dollars for cancer research; 12% of the funds went to breast cancer, 6% to prostate cancer, and 5% to lung cancer (“National Cancer Institute”, 2011). The large investment in cancer research likely drives the emphasis on cancer in nanomedicine. Table 7 lists the most researched cancers in nanomedicine. The publication profile closely resembles that funding patterns of the NCI. The cancers with the most publications, like breast cancer, also have the most funding by the NCI.
Another reason cancer features prominently in nanomedicine is that scientists are investigating whether nanoparticles cause cancer. Some scientists worry that nanoscale fibers like carbon nanotubes may increase the risk of some types of cancer, like lung cancer, if the particles are inhaled (Stern & McNeil, 2008). Environmental, health, and safety (EHS) research of nanotechnology has grown in prominence and funding over the past 10 years(National Science and Technology Council, 2011) and the increasing emphasis on the EHS aspects of nanotechnology may increase the nanomedicine research on cancer.
Two main uses of nanomedicine for cancer treatment are drug delivery systems and cancer detection systems (Nie, Xing, Kim, & Simons, 2007). Scientists are inventing better drug delivery systems in order to target cancerous cells more directly. If scientists can improve drug delivery systems, they can increase the effectiveness of the drugs and decrease the side effects of cancer treatment. For cancer detection, scientists hope that nanotechnology will enable early detection of the cancerous cells so that the disease can be treated earlier in its development which will reduce the mortality rate of cancers (Ferrari, 2005).
Alzheimer’s, the second most researched topic in WoS, is the 6th most common cause of death for developed countries. Like cancer, there is significant funding and advocacy to support Alzheimer’s research (Alzheimer’s Association, 2012). But unlike cancer Alzheimer’s is not one of the top ten causes of death. Rather, Alzheimer’s disease is only a leading cause of death in very high-income countries. The other “high income” diseases that receive a lot of attention from nanomedicine are diabetes, colon cancer, and stomach cancer.
In contrast to very high-income diseases, the most researched diseases for low income are diarrheal disease, HIV/AIDS, neonatal infections, tuberculosis, and malaria. Hepatitis, another major nanomedicine research area, is not one of the top killers in low-income countries but the disease disproportionately affects the poor (see Table 6).
The nanomedicine publication patterns from low-income countries are distinct from very high-income countries. While very high-income countries conduct research on all the diseases, nanomedicine research from low-income countries is focused on diseases of poverty like malaria and tuberculosis; 78% of the nanomedicine in WoS from low-income countries are about diseases of poverty. In comparison, only 16% of nanomedicine articles from very high-income countries deal with diseases of poverty. Therefore even though low-income countries produce far fewer nanomedicine publications than very high-income countries, their research profiles are geared towards diseases that affect their population. Another trend among low-income countries is that they collaborate more than high-income countries; 78% of the nanomedicine articles from low-income countries in WoS were “northsouth” collaborations. On the other hand a small percentage of collaborations in very high-income countries were with the global south. The data suggests that low-income countries rely on collaboration with rich countries in order to produce researched indexed in WoS or PubMed.
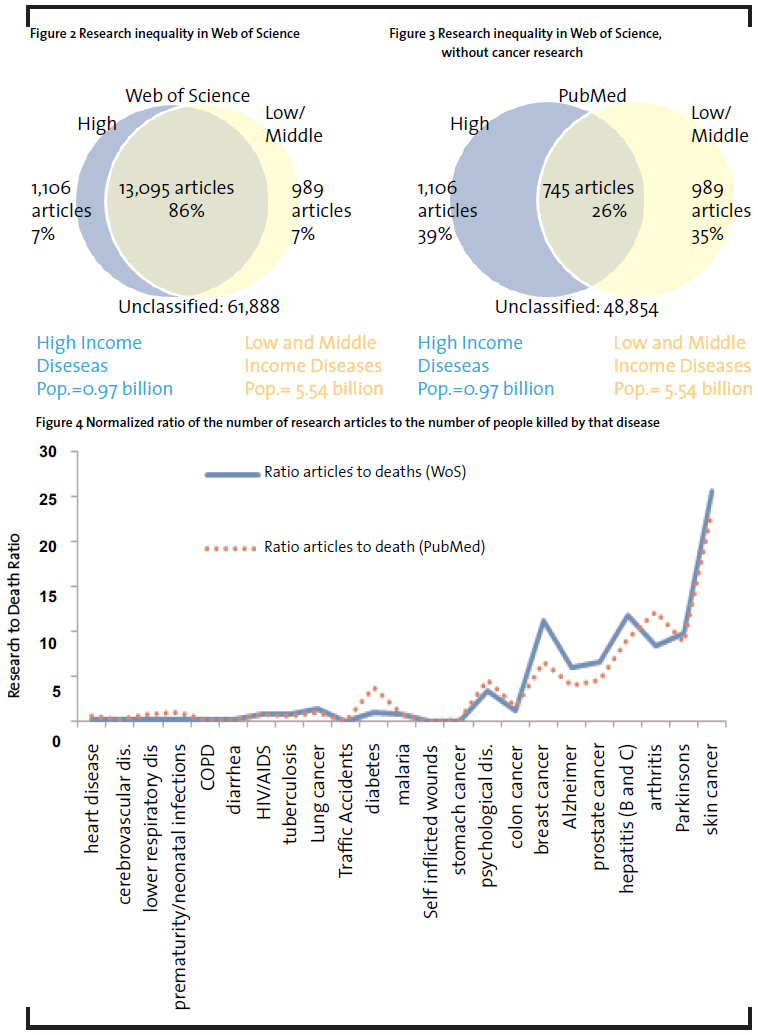
Overall in WoS (Figure 2) about 86% of the nanomedicine research impacts both rich and middle/low income countries; 7% of the research is directed towards problems of the rich and 7% is directed towards problem of middle/low income countries. A significant amount of the research that will help both rich and poor relates to cancer; 88% of the “pro-poor” research is cancer research. Even when cancer is removed from the dataset, the data still shows that nanomedicine research is balanced between country income groups (Figure 3)1. Finally, when the publication profile is examined based on population, there is not any inequality in nanomedicine research. About 5.7 billion or 82% of the world’s population live in middle/low income countries and 93% of nanomedicine research will benefit this population. Most of that benefits the poor is about cancer, however, there is significant research on malaria, tuberculosis, and HIV/AIDS.
4.4 Inequality in Disease Burden
The top ten leading causes of death accounted for 30 million deaths or 50% in 2004. The total amount of directed nanomedicine research on these deadly diseases is 10% in WoS and 19% in PubMed. Hence diseases that account for half the world’s death receive between 10% and 19% of research. This suggests that is a 20/50 gap: Less than 20% of nanomedicine research goes to solving problems that account for 50% of the global disease burden. Though this statistic shows that there is inequality in nanomedicine research, it is not as bad as a 10/90 gap.
Some diseases kill relatively few people each year but they receive a lot of attention from researchers; these diseases are over-researched. On the other hand, some diseases are under-researched; these diseases have high mortality rates yet are not heavily researched. Figure 4 shows the disease research to death ratio of several diseases. If the disease to death ratio is less than 1, then scientists are spending less time researching the disease relative to its mortality rate. On the other hand, if the disease to death ratio is greater than 1, then researchers are spending more time studying a disease compared to its mortality rate. Six diseases, diarrhea, COPD, lower respiratory disease, cerebrovascular disease, heart disease, and prematurity/low birth weight in infants receive significantly less research than they deserve2. On the other hand, cancer, hepatitis, Alzheimer’s, Parkinson’s disease, and arthritis receive more attention than is warranted. Hepatitis publications are about 3% of all directed nanomedicine research, but it only kills about 0.3% of the world’s population. The disease ratio to research ratio for the three major diseases of poverty, tuberculosis, HIV/AIDS, and malaria are not heavily skewed. The research to death ratio for these diseases range from 0.65% to 0.9%. This shows that scientists are devoting sufficient amount of attention to these diseases and that overall there isn’t research inequality for these diseases.
5 Discussion
This paper gives a descriptive analysis of nanomedicine research and classifies whether there is inequality in the research. Overall twenty percent of all nanotechnology articles are related to nanomedicine and in WoS the percent of nanomedicine articles has grown over the past 10 years. Nanomedicine is growing in importance and scientists are developing new medicines to address many of the world’s diseases.
This study has three hypotheses. The first hypothesis is that nanomedicine is predominantly conducted in very high-income countries. The data supports this hypothesis. About 77% of nanotechnology research is conducted in very high-income countries but these countries only contain 15% of the world’s population. However, over the next few decades, it is possible that the trend will change. Medium income countries like China and India are becoming world leaders in nanotechnology and they are rivaling countries with very high incomes in nanomedicine research. The second hypothesis is that there is a disproportionate amount of nanotechnology research conducted on diseases of very high-income countries. There is no evidence to support this hypothesis. Scientists are doing nanomedicine research on a variety of diseases that affect both the rich and the poor. Although diseases of the rich like Alzheimer’s and breast cancer receive the most attention, diseases like tuberculosis, malaria, and HIV/AIDS also receive some attention from nanomedicine scientists. The disease with the most nanomedicine publications is cancer. Cancer is a leading killer in high-income countries, but currently, cancer is not a top disease in middle and poor countries. However as people in poor countries get richer and have longer life expectancies, cancer will become a more serious problem.
The third hypothesis is that the majority of nanomedicine research only addresses diseases that kill relatively few people. This hypothesis is partially confirmed. Several diseases like skin cancer, hepatitis, breast cancer, Parkinson’s, and arthritis are over-researched. These diseases cause relatively few deaths yet they receive a lot of attention from scientists. Nevertheless, there are several diseases like diarrhea disease, COPD, and infant death due to prematurity and low birth weight do not receive enough attention from scientists. However, there are many diseases of poverty, like malaria, HIV/AIDS, and tuberculosis that do receive enough attention in relation to the number of people the diseases kill. Moreover, there is a 20/50 gap in nanomedicine: less than 20% of nanomedicine research goes to solving diseases that account for 50% of deaths.
There are several limitations to this study. First, the study uses Web of Science and PubMed to quantify inequality in nanomedicine. Though these databases are often used in bibliometric studies they have small biases. These databases tend to have a higher representation of English journals and they tend to have more journals from high-income countries (UNESCO, 2005). As a result, research from developing countries may be underrepresented in the dataset. Also, this study cannot determine whether the articles were discussing how nanotechnology can cure diseases, cause more diseases or provide patients with more access to nanomedicine. This is especially significant when analyzing cancer. Scientists study both how nanotechnology can fight cancer (Ferrari, 2005) and how it could potentially cause cancer (Stern & McNeil, 2008). As a result, some of the nanomedicine papers may focus on toxicology as opposed to fighting cancer. Finally, many of the top “diseases” do not have much overlap with nanomedicine. For example, traffic accidents are the ninth leading cause of death, and self-inflicted injuries are the sixteenth leading cause of death. It is doubtful that nanomedicine will impact those areas.
From this study, it is hard to conclude why nanomedicine does not have large research inequalities like those reported in other medical fields. One potential cause is that the research profile is heavily influenced by funding agencies that sponsor disease-specific nanomedicine. 15% of the WoS articles in the nanomedicine dataset attribute to a funding sponsor. Most of the sponsored research is attributed to large government research funding organizations like the USA National Institutes of Health (NIH). Since cancer is a major focus area for the NIH, scientists may be drawn to cancer research in order to get research money. Other factors that affect scientist motivations may like organizational structure and reward system (Fox, 1983).
This study is the first step in understanding inequality in nanomedicine and adds to the discussion on the 10-90 gap. It shows that scientists are studying how emerging technologies, like nanotechnology, can benefit the poor and that many of the inequality trends that existed in research and technology are changing. In the future scholars can add information about whether nanomedicine affects health inequality based on disability-adjusted life years (DALY). DALY’s is an alternative measure of the burden of disease that captures the disease burden based on the years of life lost resulting from premature death and the loss resulting from losing the full quality of health (World Health Organization, 2008). By studying inequality with DALY we can understand the effects of nanomedicine on non-fatal diseases. Moreover, scholars need to understand why nanomedicine is not following the pattern of other medical research. Is there a reason that nanomedicine is not following the same 10-90 gap that is apparent in other medical fields?
Moral philosophies and belief systems view inequality as bad for society (S. E. Cozzens, 2007). Science and technology can play a crucial role in diminishing inequality however science and technology do not automatically reduce inequality (Woodhouse & Sarewitz, 2007). If the technology is not introduced correctly it can lead to greater inequalities as seen in other areas of medical technologies. The chemicals industry plays a crucial role in nanomedicine. Although it may not be directly involved in choosing the research portfolio for researchers, the chemical industry plays a big part of providing supplies, equipment, and expertise for the technology. The research in nanomedicine will influence where companies should operate and what type of nanotechnology products it should offer to consumers. By understanding the research in nanomedicine, the field will be able better respond to customer demand.
Acknowledgments:
I would like to thank Susan Cozzens, Jan Youtie, Diana Hicks, Alan Porter and the reviewers for their comments on this paper. I would also like to that researcher at the Center for Nanotechnology and Society at the Georgia Institute of Technology for letting me use their nanotechnology database. This study was funded by the National Science Foundation, Graduate Student Fellowship and NSF award #0937591.
References
Alzheimer’s Association. (2012): Alzheimer’s Association: Research, http://www.alz.org/research/, accessed 10 July 2012
Balogh, L. P. (2010): Why do we have so many definitions for nanoscience and nanotechnology?, Nanomedicine: nanotechnology, biology, and medicine, 6(3), p. 397-8.
Cozzens, S. E. (2007): Distributive Justice in Science and Technology Policy, Science and Public Policy, 34(2), p. 85-94.
Cozzens, S., Gatchair, S., Kang, J., Kim, K.-S., Lee, H. J., Ordóñez, G., & Porter, A. (2010): Emerging technologies: quantitative identification and measurement, Technology Analysis & Strategic Management, 22(3), p. 361-376.
Doyal, L. (2004): Gender and the 10/90 gap in health research, Bulletin of the World Health Organization, 82(3), p. 162.
ETC Group. (2006): Medical Applications of Nano-scale Technologies: What Impact on Marginalized Communities? Ottawa: ETC Group, http://www.etcgroup.org/en/materials/publications.html?pub_id=593
Falagas, M. E., Karavasiou, A. I., & Bliziotis, I. a. (2006): A bibliometric analysis of global trends of research productivity in tropical medicine, Acta tropical, 99(2-3), p. 155-9.
Ferrari, M. (2005): Cancer nanotechnology: opportunities and challenges, Nature Reviews Cancer, 5(3), p. 161– 171. Nature Publishing Group.
Fox, M. F. (1983): Publication Productivity among Scientists: A Critical Review, Social Studies Of Science, 13(2), p. 285-305.
Global Forum for Health Research. (2004): The 10/90 Report on Health Research 2003-2004. Development. Geneva, Switzerland.
Guan, J., & Ma, N. (2007): China’s emerging presence in nanoscience and nanotechnology A comparative bibliometric study of several nanoscience “giants.”, Research Policy, 36(6), p. 880-886.
Hassan, M. H. A. (2005): Small Things and Big Changes in the Developing World, Science, 309(July), p. 65-66.
Huang, L., Peng, Z., Guo, Y., & Porter, A. L. (2010): Identifying the emerging roles of nanoparticles in biosensors. Journal of Business Chemistry, 7(1).
Invernizzi, N., & Foladori, G. (2006): Nanomedicine, Povertyand Development, Development, 49(4), p. 114.
Leydesdorff, L. (2008): Caveats for the use of citation indicators in research and journal evaluations. Journal of the American Society for Information, 59(2), p.1-31.
Liu, X., Zhang, P., Li, X., Chen, H., Dang, Y., Larson, C., Roco, M., et al. (2009): Trends for nanotechnology development in China, Russia, and India, Journal of Nanoparticle Research, 11(8), p. 1845-1866.
Mari, J. J., Patel, V., Kieling, C., Razzouk, D., Tyrer, P., & Herrman, H. (2010): The 5/95 gap in the indexation of psychiatric journals of low- and middle-income countries. Acta psychiatrica Scandinavica, 121(2), p. 152-6.
Martini, N., Tomino, C., Liberati, A., Carpenter, K. J., Roberts, S., & Sternberg, S. (2003): Research gap in cardiovascular disease in developing countries, The Lancet, 361, p. 2246-2247.
Meridian Institute. (2006): Nanotechnology, Water, and Development, 51(2). Chennai, India.
Médecins Sans Frontières. (2001): Fatal Imbalance: The Crisis in Research and Development for Drugs for Neglected Diseases, (8405). Geneva, Switzerland.
National Cancer Institute. (2011): http://www.cancer.gov/, accessed 31 March 2011
National Center for Biotechnology Information. (2012): PubMed. , http://www.ncbi.nlm.nih.gov/pubmed, accessed 11 June 2012
National Science and Technology Council. (2011): National Nanotechnology Initiative: Strategic Plan. Washington D.C., www.nano.gov
Nie, S., Xing, Y., Kim, G. J., & Simons, J. W. (2007): Nanotechnology applications in cancer, Annual review of biomedical engineering, 9, p. 257-88.
Niosi, J., & Reid, S. E. (2007): Biotechnology and Nanotechnology: Science-based Enabling Technologies as Windows of Opportunity for LDCs? World Development, 35(3), p. 426-438.
OECD. (2005): Opportunities and risks of Nanotechnologies. Paris, France.
PCAST. (2010): Report to the President and Congress on Third Assement on the National Nanotechnology Initiative. Washington D.C.
Pastrana, T., Vallath, N., Mastrojohn, J., Namukwaya, E., Kumar, S., Radbruch, L., & Clark, D. (2010): Disparities in the contribution of low- and middle-income countries to palliative care research, Journal of pain and symptom management, 39(1), p. 54-68.
Porter, A., Youtie, J., Shapira, P., & Schoeneck, D. (2007): Refining Search Terms for Nanotechnology, Journal of Nanoparticle Research, 10(5).
Ramani, S. V., Chowdhury, N., Roger, C., & Reid, S. E. (2010): On India’s Plunge into Nanotechnology: What are good ways to catch-up. Globelics 2010 Malaysia, http://umconference.um.edu.my/upload/43-1/papers/189ShyamaRamani_ NupurChowdhury_RogerCoronini_SusanReid.pdf
Reich, M. R. (2000): The global drug gap, Science, 287(5460), 1979.
Roco, M. C., & Bainbridge, W. S. (2005): Societal implications of nanoscience and nanotechnology: maximizing human benefit, Journal of Nanoparticle Research, 7(1), p. 1-13.
Sahoo, S., Parveen, S., & Panda, J. (2007): The present and future of nanotechnology in human health care, Nanomedicine: Nanotechnology, Biology and Medicine, 3(1), p. 20–31.
Silva, G. A. (2004): Introduction to nanotechnology and its applications to medicine, Surgical neurology, 61(3), p. 216–220.
Stern, S. T., & McNeil, S. E. (2008): Nanotechnology safety concerns revisited, Toxicological sciences: an official journal of the Society of Toxicology, 101(1), p. 4-21.
Stevens, P. (2007): Diseases of poverty and the 10/90 Gap. In Philip Stevens (Ed.), Fighting the Diseases of Poverty. London: International Policy Press., http://sarpn.org/documents/d0002617/6 -Disease_Poverty_IPN_2007.pdf
Thomson Reuters. (2012): Web of Science – IP & Science., http://wokinfo.com/products_tools/multidisciplinary/webofscience/, accessed 11 June 2012
UNESCO. (2005): What do Bibliometric Indicators Tell Us About World Scientific Output? (2). Montreal: UNESCO.United Nations. (2010a): The United Nations at a Glance. New York: United Nation., http://www.un.org/en/aboutun/index.shtml
United Nations. (2010b): UN-Human Development Index.,http://hdr.undp.org/en/reports/global/hdr2010/chapters/en/, accessed 31 March 2011
Wagner, V., Dullaart, A., Bock, A. K., & Zweck, A. (2006): The emerging nanomedicine landscape, Nature Biotechnology, 24(10), p. 1211–1218.
Woodhouse, E., & Sarewitz, D. (2007): Science policies for reducing societal inequities, Science & Public Policy (SPP), 34(2), p. 139-150.
World Health Organization. (2008): The Global Burden of Disease 2004. Geneva, Switzerland.
Zawislak, P. A., Marques, L. F., Esteves, P., & Rublescki, F. (2010): Technological trajectories and multidimensional impacts: further remarks on the nanotechnology industry. Journal of Business Chemistry, 7(1).